For Healthcare Professionals
Home Health Care
Home Health Care helps patients to recover from injury, illness, a medical procedure, or cope with a chronic illness within the comfort of their home. Home health care likewise aids in promoting health improvement, quality of life, independence, and prevention of unnecessary re-hospitalization of patients.
Home Health Care Eligibility
General Eligibility Guidelines
One must satisfy the criteria developed by the Centers for Medicare and Medicaid services, as listed below, in order to be eligible for home care:
- Patient is homebound per the advice of the physician.
- Patient is cared for by a physician and receives services reviewed by a doctor on a regular basis.
- The Home Health Care agency must be Medicare-certified.
- Patient’s physician should certify the patient’s need for any of the following, but not limited to: Intermittent skilled nursing care, physical therapy, speech-language pathology services, and continued occupational therapy.
- A physician or a healthcare professional that works with the doctor must document a face-to-face encounter within a specified time and the encounter must be related to the patient’s need for home health care.

Hospice Care
Hospice is a service provided by an interdisciplinary care team to any patient who is diagnosed with a terminal illness and certified by a physician that they have less than six months to live. While traditional medical care focuses on treating disease and illness, hospice care centers on improving the quality of life for the individual, in addition to providing support and education to the family. Hospice care provides a team-oriented approach to delivering medical care, pain management, and emotional and spiritual support individualized to the patient’s needs and wishes. The service is provided where the patient resides, at home or in a facility. At Care Dimensions Healthcare, our mission is to provide compassionate, quality care with respect and comfort to our patients and their families/caregivers.
Hospice Care Eligibility
- General Eligibility Guidelines
One must satisfy the criteria developed by the Centers for Medicare and Medicaid services, as listed below, in order to be eligible for hospice care:
- The Hospice Care agency must be Medicare-certified.
- The attending physician (if they have one) and the hospice physician must certify the patient as terminally ill with a medical prognosis of 6 months or less to live if the illness runs its normal course.
- The patient must sign an election statement to elect the hospice benefit and waive all rights to Medicare payments for the terminal illness and related conditions.
- A physician or a healthcare professional that works with the doctor must document a face-to-face encounter within a specified time and the encounter must be related to the patient’s need for home health care.
- Non Disease Specific Guidelines
If a patient meets at least 2, consider Hospice:
- Palliative Performance Score (PPS) less than 70%
- Dependence on 2 or more Activities of Daily Living (ADLs)
- SOB at rest or with minimal exertion
- Multiple ER visits or hospitalizations
- Recurrent falls with injury
- Weight loss of 10% or more in last 6 months
- Presence of the following Comorbidities, the severity of which is likely to contribute to the life expectancy of 6 months or less:
- Cancer
- COPD
- CHF
- Liver Disease
- Ischemic Heart Disease
- Neurologic Disease (CVA, ALS, MS, Parkinson’s)
- Type 2 Diabetes Mellitus (DM)
- Renal Failure
- HIV/AIDS
- Dementia/Alzheimer’s
- Refractory severe autoimmune disease (Lupus or Rheumatoid Arthritis)
These guidelines are provided as a reference tool but do not take the place of a physician’s professional judgment.
- Disease Specific Guidelines
- Cancer
Use in conjunction with “Non Disease Specific Guidelines”.
- Patient declines further chemotherapy/immunotherapy
- Cancer has metastasized
- Continued decline in spite of therapy
- Certain cancers with poor prognosis may be hospice eligible without fulfilling the other criteria in this section
- Neurological Diseases (Amyotrophic Lateral Sclerosis/ Lou Gehrig’s Disease (ALS), Multiple Sclerosis, Non-Alzheimer’s Dementia, Parkinson’s, Huntington’s disease, etc.).
Use in conjunction with “Non Disease Specific Guidelines”.
- Inability to swallow liquids or soft food without choking or coughing
- Inability to clear respiratory secretions, persistent cough, recurrent aspiration pneumonia, and severely compromised breathing
- Impaired communication marked by barely intelligible speech
- Patient/family declines to continuation of a feeding tube or ventilator/tracheostomy
- Alzheimer’s Disease
Use in conjunction with “Non Disease Specific Guidelines”.
- All of the following characteristics present:
- FAST Stage of 7a or above
- Unable to dress without assistance
- Unable to bathe without assistance
- Unable to ambulate without assistance
- Urinary and Fecal incontinence
- Loss of basic motor skills
AND
- At least 1 of the following within the past year:
- Aspiration pneumonia
- Septicemia
- Pyelonephritis
- Decubitus Ulcer, Multiple stage 3‐4
- Fever, recurrent after a course of antibiotics
- 10% weight loss in 6 months or decreased serum albumin < 2.5 gm/dl
Stage
Characteristics
1-6
Not eligible
7a
Speaks <= 6 words during the day
7b
Speaks one intelligible word during the day
7c
Ability to ambulate is lost
7d
Not able to sit up without assistance
7e
Ability to smile is lost
7f
Ability to hold up head independently is lost
- Heart Diseases (Congestive Heart Failure, CAD, Cardiomyopathy, Ischemic Heart Disease, Myocardial Infarction, Hypertensive Heart Disease, Valvular Heart Disease, etc.)
Use in conjunction with “Non Disease Specific Guidelines”.
- Optimally treated with vasodilators and diuretics
- For CHF and Angina ‐ New York Heart Association (NYHA) Class IV (Unable to carry out any physical activity without discomfort. Symptoms of cardiac insufficiency at rest. If any physical activity is undertaken, discomfort is increase)
- May need supportive documentation, but NOT required:
- EF of < 20%
- History of cardiac arrest or resuscitation
- Treatment resistant symptomatic supraventricular or ventricular arrhythmias
- History of unexplained syncope Brain embolism of cardiac origin
- HIV/AIDS
Use in conjunction with “Non Disease Specific Guidelines”.
- CD4+ <25 cells/mcl or Persistent viral load > 100,000 copies/ml plus any of the following:
- CNS Lymphoma (untreated/treatment resistant)
- Wasting (loss of at least 10% of lean body mass)
- Progressive multifocal leukoencephalopathy
- Mycobacterium avium complex bacteremia
- Systemic lymphoma with advanced HIV disease
- Visceral Kaposi’s sarcoma
- Renal failure in the absence of dialysis
- Cryptosporidium infection
- Toxoplasmosis
- Palliative performance scale (PPS) ≤ 50%
- May need supportive documentation, but NOT required:
- Chronic persistent diarrhea for 1 year
- Concomitant, active substance abuse
- Persistent serum albumin < 2.5 gm/dL
- Age > 50 years
- Advances AIDS dementia complex
- Absence/resistance to effective therapy
- Toxoplasmosis
- CHF, symptomatic at rest, NYHA Class IV
- Advance Liver Disease
- Liver Disease (Chronic Hepatitis, Liver Cirrhosis, Biliary Cirrhosis, Hepatic Fibrosis, Hepatic Encephalopathy, etc.)
Use in conjunction with “Non Disease Specific Guidelines”.
- Patient should have both:
- PT prolonged > 5 secs over control or INR > 1.5
- Serum Albumin < 2.5 gm/dL
- And at least 1 of the following present:
- Ascites
- Spontaneous Bacterial Peritonitis
- Hepatic Encephalopathy
- Hepatorenal Syndrome
- Recurrent Variceal bleeding
- May need supportive documentation, but NOT required:
- Progressive malnutrition
- Muscle wasting with reduced strength and endurance
- Hepatocellular carcinoma
- Continued active alcoholism (> 80 gm Ethanol/day)
- HBsAG (Hepatitis B positivity)
- Hepatitis C refractory to interferon treatment
- Pulmonary Disease (Chronic Bronchitis, COPD, Emphysema, Respiratory Failure, Pulmonary Fibrosis, etc.)
Use in conjunction with “Non Disease Specific Guidelines”.
- Patient should have both:
- Disabling dyspnea at rest, poorly or unresponsive to bronchodilators (Decreased FEV1 optional)
- Increasing visits to the ED or hospitalizations for pulmonary infections/respiratory failure
- Hypoxemia or Hypercapnia at rest and on room air (pO2 ≤ 55mm HG OR Oxygen saturation ≤ 88% OR pCO2 ≤ 55 mm Hg)
- May need supportive documentation:
- Right heart failure secondary to Cor Pulmonale
- Unintentional weight loss > 10% body weight in 6 months
- Resting tachycardia > 100/min
- Renal Disease
Use in conjunction with “Non Disease Specific Guidelines”.
- Patient is not seeking dialysis or renal transplant (Note: ESRD benefit is separate from Hospice benefit; Patients can avail of both the Hospice benefit and the ESRD benefit when the need for dialysis is NOT RELATED to the patient’s terminal condition.)
- And at least 1 of the following present:
- Creatinine level < 10 mL/min (<15 mL/min id with DM) or < 15 mL/min if with CHF (<20 mL/min if with DM)
- Serum Creatinine > 8.0mg/dL (>6.0 mg/dL if with DM)
- Estimated GFR <10 mL/min
- May need supportive documentation:
- Mechanical ventilation
- Malignancy of other organ system
- Chronic Lung Disease
- Advanced cardiac or liver disease
- Immunosuppression/ AIDS
- Albumin < 3.5 gm/dL
- Platelet count < 25,000
- Disseminated Intravascular Coagulation
- Stroke/CVA/Coma (Hemiplegia or Generalized Muscle Weakness with or without Dysphagia as a late effect of CVA, Thromboembolic Stroke, Intracerebral Hemorrhage, Subdural Hematoma, Aneurysmal Bleed, etc.)
Use in conjunction with “Non Disease Specific Guidelines”.
- PPS Score of < 40%
- And at least 1 of the following present:
- Weight loss > 10% in 6 months or > 7.5% in 3 months
- Pulmonary Aspiration
- Serum Albumin < 2.5gm/dL
- Inadequate intake by sequential calorie count
- Severe dysphagia
- Coma of any etiology or coma patient with any 3 of the following on day 3 of the coma:
- Abnormal brainstem response
- Absent verbal response
- Serum Creatinine > 1.5 mg/dL
- Absent withdrawal response to pain
- May need supportive documentation:
- Medical complications
- Progressive clinical decline for past 1 year
- Aspiration pneumonia
- Refractory Stage 3‐4 decubitus ulcers
- Pyelonephritis
Palliative Performance Scale (PPS)
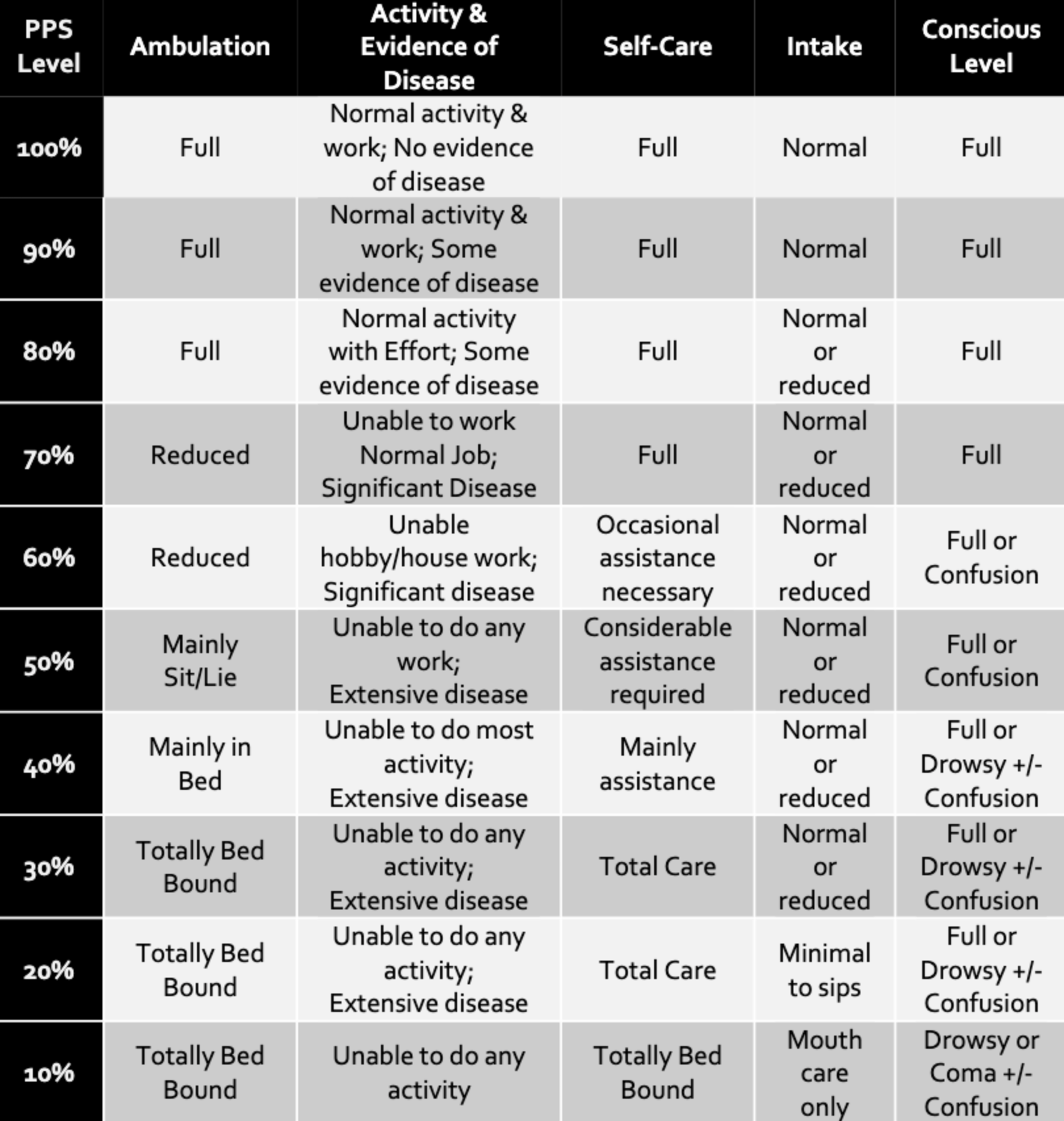
These guidelines are provided as a reference tool but do not take the place of a physician’s professional judgment.
Palliative Care
Palliative care is a service that focuses on symptom management, comfort, and quality of life for individuals with chronic injury, illness, or disease such as stroke, heart failure, or cancer. Individuals can qualify to receive the care at the time of diagnosis and during curative care efforts. The focus is on providing comfort for the time being rather than prolonging life. An example of palliative care is pain and symptom management related to multiple sclerosis. Palliative care can be provided along with curative treatment. Over time, however, if the doctor and/or the palliative care team believe that the treatment is no longer helping, the doctor may recommend hospice.
- General Eligibility Guidelines
The patient must meet all of the general eligibility criteria.
- Is likely to or has started to use the hospital or emergency department as a means to manage the patient’s advanced disease (this refers to unanticipated decompensation and does not include elective procedures.
- Has an advanced illness, as defined in the Section for Disease Specific Eligibility below, with appropriate documentation of continued decline in health status and is not eligible for or declines hospice enrollment.
- Death within a year would not be unexpected based on clinical status.
- Has received appropriate patient-desired medical therapy OR is a patient for whom patient-desired medical therapy is no longer effective. The patient is NOT in reversible acute decompensation.
- The patient and the family/patient-designated support (if applicable) agrees to:
- Attempt, as medically/clinically appropriate, in-home, residential-based, or outpatient disease management/palliative care instead of going to the emergency department first; and
- Participate in Advance Care Planning discussions.
- Disease Specific Guidelines
The patient must meet at least one of the four disease-specific eligibility criteria. (If the patient is younger than 21 years old, see Pediatric Palliative Care Eligibility section.)
- Congestive Heart Failure (CHF)
- Patient should have both:
- The patient is hospitalized due to CHG as the primary diagnosis with no further invasive interventions planned or meets criteria for the New York Heart Association’s (NYHA) heart failure classification III or higher.
- The patient has an ejection fraction of less than 30% for systolic failure OR significant comorbidities.
- Chronic Obstructive Pulmonary Disease (COPD)
- Patient should have both:
- The patient has a forced expiratory volume (FEV) of 1 less than 35% of predicted AND a 24-hour oxygen requirement of less than 3 liters per minute.
- The patient has a 24-hour oxygen requirement of greater than or equal to 3 liters per minute.
- Cancer
- Patient should have both:
- The patient has stage III or IV solid organ cancer, lymphoma, or leukemia.
- The patient has a Karnofsky Performance Scale score less than or equal to 70% OR has failure of two lines of standard of care therapy (chemotherapy or radiation therapy).
- Liver Disease
- Patient should have both:
- The patient has stage III or IV solid organ cancer, lymphoma, or leukemia.
- The patient has a Karnofsky Performance Scale score less than or equal to 70% OR has failure of two lines of standard of care therapy (chemotherapy or radiation therapy).
- Or at least 1 of the following:
- The patient has evidence of irreversible liver damage and has a Model for End-Stage Liver Disease (MELD) score of greater than 19.
- The patient has evidence of irreversible liver damage, serum albumin less than 3.0, an International Normalized Ratio (INR) greater than 1.3.
- Patient should have both:
- Patient should have both:
- Patient should have both:
- Patient should have both:
- Stroke/CVA
- The patient is unable to take oral nutrition, change in mental status, history of aspiration or aspiration pneumonia.
- Chronic Kidney Disease (CKD) or End-stage Renal Disease (ESRD)
- Severe Dementia or Alzheimer’s Disease
- Pediatric Palliative Care Eligibility
The patient must meet all of the general eligibility criteria.
- General Eligibility Guidelines
- Patient should have both:
- The patient is under the age of 21
- The family and/or legal guardian agrees to the provision of pediatric palliative care services.
- Disease Specific Eligibility Guidelines
- The patient must meet at least one of the four disease-specific eligibility criteria
- Conditions for which curative treatment is possible, but may fail (e.g. advanced or progressive cancer or complex and severe congenital or acquired heart disease)
- Conditions requiring intensive long-term treatment aimed at maintaining quality of life (e.g. human immunodeficiency virus infection, cystic fibrosis, or muscular dystrophy)
- Progressive conditions for which treatment is exclusively palliative after diagnosis (e.g. progressive metabolic disorders or severe forms of osteogenesis imperfecta)
- The patient must meet at least one of the four disease-specific eligibility criteria
- Patient should have both:
Conditions involving severe, non-progressive disability, or causing extreme vulnerability to health complications (e.g. extreme prematurity, severe neurologic sequelae of infectious disease or trauma, severe cerebral palsy with recurrent infection or difficult-to-control symptoms)